In cases where the clinical picture alone is insufficient to guide treatment, CT plaque analysis serves as a powerful tie-breaker — moving the decision from population-level risk estimates to a direct assessment of what is occurring inside an individual patient's arteries. When results reveal no significant plaque, this provides objective evidence that the patient's arterial health is better than their risk factors alone might suggest. This finding can reasonably support a decision to defer or withhold statin therapy, while offering meaningful reassurance to both the patient and their clinician.
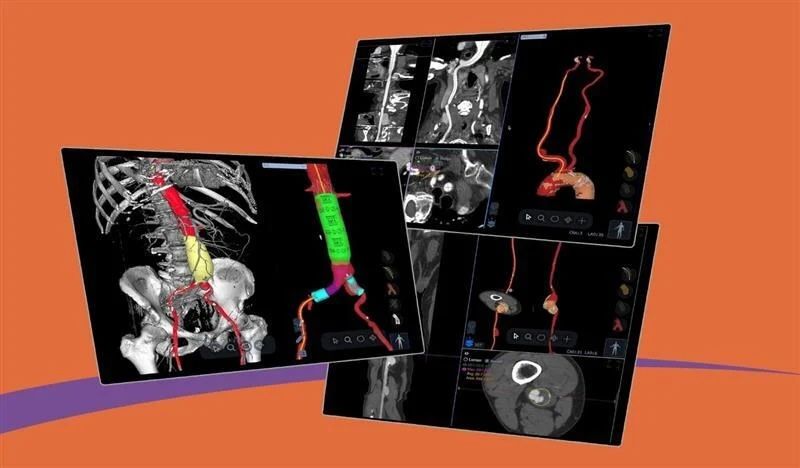
New solution brings advanced vascular analysis into the cvi42 cardiovascular imaging ecosystem. Highlights Circle Cardiovascular Imaging (Circle CVI) has expanded its cvi42 platform to include advanced Vascular CT analysis, integrating Astute Imaging’s AI-driven vascular analysis technology. This enhancement enables comprehensive cardiovascular workflows, allowing clinicians to perform cardiac, vascular, and structural heart analysis within a single, unified platform. This integration supports greater efficiency and collaboration across cardiology, radiology, and vascular surgery teams, advancing the use of quantitative, AI-enabled imaging for diagnosis, procedural planning, and post-treatment management Calgary, AB — March 18, 2026 — Circle Cardiovascular Imaging (Circle CVI) today announced the expansion of its cvi42 cardiovascular imaging platform to include advanced Vascular CT analysis, further extending the platform’s capabilities across cardiovascular imaging workflows. The new solution is enabled through a collaboration with Astute Imaging, whose AI-driven vascular analysis technology has been integrated into the cvi42 ecosystem. The addition of Vascular CT capabilities allows clinicians to analyze complex vascular anatomy for diagnosis, endovascular procedure planning, and post-treatment surveillance, all within the same platform used for cardiac imaging and structural heart planning. Advancing Quantitative Cardiovascular Imaging As healthcare systems increasingly adopt quantitative imaging and AI-enabled workflows, clinicians are seeking integrated platforms that can support the full continuum of cardiovascular care — from diagnosis to procedural planning and long-term disease management. The new Vascular CT capabilities extend the scope of cvi42 beyond cardiac imaging, enabling automated vascular analysis within the same environment trusted by cardiovascular teams worldwide. The technology powering these capabilities was developed by Astute Imaging, whose advanced algorithms support automated segmentation, quantification, and visualization of vascular structures. “Fragmented imaging workflows can slow collaboration and decision making between cardiovascular teams,” said Dr. Kevin Steel, Chief Medical Officer, Circle CVI. “By bringing vascular CT analysis into the cvi42 ecosystem, clinicians can work from the same platform across cardiac and vascular cases, helping improve efficiency and coordination of care.” Cardiac and vascular analysis within a unified workflow helps multidisciplinary cardiovascular teams collaborate more effectively across cardiology, radiology, and vascular surgery. ABOUT CIRCLE CARDIOVASCULAR IMAGING Circle Cardiovascular Imaging Inc. (Circle CVI) is a Canadian-based company founded in 2007 with a mission to develop innovative software solutions that enhance cardiovascular and cerebrovascular imaging analysis and ultimately improve patient care. Circle’s flagship platform, cvi42 , delivers best-in-class image reading and reporting tools for quantitative and qualitative assessment of cardiac MR, cardiac CT, vascular CT, and neuro CT . At the core of Circle’s work is a relentless commitment to empowering healthcare providers with advanced, intuitive tools that lead to better healthcare outcomes. This passion for innovation, rooted in both medicine and technology, drives Circle’s global impact and fuels a culture of excellence. Today, millions of medical imaging exams each year, across 1,700+ hospitals in over 90 countries, are interpreted using Circle’s cvi42 platform. For more information, please visit www.circlecvi.com or contact: marketing@circlecvi.com About Astute Imaging Astute Imaging Inc. is a U.S.-based company founded in 2022 with a mission to become a best-in-class provider of AI-enabled vascular imaging and care management software for healthcare providers and MedTech companies. Astute Imaging delivers a fully automated, AI-enabled workflow supporting diagnostics, surgical planning, and longitudinal patient follow-up. The platform covers all major vascular anatomies, including the aorta, carotid arteries, and peripheral vasculature. In addition, Astute Imaging provides AI-enabled virtual device simulation, allowing surgeons to visualize and automatically identify the most appropriate device for a patient’s anatomy, enabling highly personalized procedural planning and care management. Astute Imaging’s technology is also used by medical device companies for regulatory and research applications, including core lab services and R&D support. For media inquiries, please contact: marketing@astuteimaging.com
Coverage unlocks reimbursable AI plaque quantification, advancing coronary risk assessment in everyday cardiology practice. Highlights New permanent Category I CPT code 75577 for AI-enabled coronary plaque analysis took effect January 1, 2026 Major payers, including Aetna, alongside UnitedHealthcare, Cigna, Humana, and others, now cover AI-enabled coronary plaque analysis, extending access to tens of millions of commercially insured patients Circle’s FDA-cleared, on-premise cvi 42 |Plaque solution integrates directly into CCTA workflows, giving physicians hands-on control of AI plaque analysis and retains more of the plaque analysis reimbursement Calgary, Alberta – Circle Cardiovascular Imaging Inc. (Circle CVI), the market leader in cardiovascular imaging postprocessing, announced that clinical practices using its FDA 510(k)-cleared cvi 42 with AI-enabled plaque analysis solution are well positioned to benefit from newly activated reimbursement for AI-enabled coronary plaque analysis under permanent Category I CPT code 75577, effective January 1, 2026. Major insurance companies have also announced that they are also reimbursing the costs of this analysis. New Category I CPT Codes Now in Effect Beginning January 1, 2026, AIdriven quantification and characterization of coronary atherosclerotic plaque derived from coronary CT angiography (CCTA) is reimbursed under a permanent Category I CPT code, 75577, replacing prior Category III codes. This transition enables nationally valued payment for quantitative plaque assessment across hospital outpatient departments, imaging centers, and physician offices. Growing Payer Support for AI Plaque Analysis Major commercial payers, including Aetna, UnitedHealthcare, Cigna, Humana, and others, now cover AI-based quantitative coronary plaque analysis , extending access to tens of millions of commercially insured patients and building on prior Medicare coverage decisions. This expanding reimbursement is expected to accelerate adoption of CCTA-based plaque assessment. AMA/ACC Guidance on When to Use Plaque Analysis In December 2025, a major scientific statement published in the Journal of the American College of Cardiology : Cardiovascular Imaging provided consensus recommendations on how and when to use quantitative coronary plaque analysis (QCPA) in practice. Their recommendations stated that among patients who have visual evidence of plaque on coronary CTA, adding QCPA may be useful for enhancing risk assessment and guiding the initiation or intensification of preventive therapies. CCTA’s Emerging Role as a Primary CAD Modality Recent analyses from cardiovascular imaging experts highlight how CCTA, augmented by AI-enabled plaque analysis, is poised to become the foundational imaging modality for the diagnosis and management of coronary artery disease. As reimbursement stabilizes and technology matures, CCTA is increasingly viewed as the frontline test that can characterize both stenosis and atherosclerotic burden, informing preventive strategies long before invasive procedures are required. cvi42|Plaque: FDA-cleared, On-premise AI for Coronary Plaque cvi 42 |Plaque, cleared by the U.S. FDA in late 2025, is an on-premise, AI-enabled coronary plaque analysis module that integrates directly into existing cvi 42 and CCTA workflows. The software automatically segments the coronary lumen and vessel wall, quantifies plaque burden and composition, and generates structured lesion- and vessel-level metrics to support risk stratification, preventive therapy decisions, and revascularization planning. Because the solution runs locally, image data, AI processing, and reporting remain within the institution’s environment, giving physicians interactive control over contouring and final interpretation while allowing programs to retain a larger share of reimbursement compared with outsourced, cloud only services. Localized AI and Circle’s Elevate Pricing Advantage “With the new Category I CPT code for coronary plaque analysis now in effect, and the major insurance players reimbursing plaque analysis, the economics and clinical evidence are finally aligned,” said Chris Bazinet, Chief Commercial Officer at Circle CVI. “cvi 42 |Plaque gives practices an on-premise, FDA-cleared AI solution that fits directly into their existing CCTA workflows, enabling guideline consistent plaque reporting, improved risk stratification, and better capture of the reimbursement now available for quantitative coronary plaque analysis.” cvi 42 |Plaque is available as part of the broader cvi 42 platform for cardiac CT and MR. Clinical sites interested in implementing AI-enabled coronary plaque analysis can contact Circle to assess readiness, workflow integration, and revenue potential. - ENDS - About Circle Cardiovascular Imaging Circle Cardiovascular Imaging Inc. (Circle CVI) is a Canadian-based company founded in 2007 with a mission to develop innovative software solutions that enhance cardiovascular and cerebrovascular imaging analysis and ultimately improve patient care. Circle’s flagship platform, cvi 42 , delivers best-in-class image reading and reporting tools for quantitative and qualitative assessment of cardiac MR, cardiac CT, vascular CT, and neuro CT. At the core of Circle’s work is a relentless commitment to empowering healthcare providers with advanced, intuitive tools that lead to better healthcare outcomes. This passion for innovation, rooted in both medicine and technology, drives Circle’s global impact and fuels a culture of excellence. Today, millions of medical imaging exams each year—across 1,700+ hospitals in over 90 countries—are interpreted using Circle’s cvi 42 platform. For media inquiries, please contact: marketing@circlecvi.com

Highlights The latest release of cvi42v6.4 focuses on workflow efficiency and leveraging artificial intelligence In-house post-processing speeds reporting time and captures more reimbursement Circle’s vascular capabilities expand with the addition of cvi42 | Vascular CT New business models increase the flexibility and accessibility for reporting physicians Calgary, AB – Circle Cardiovascular Imaging (Circle CVI) , the market leader in cardiovascular imaging post-processing will unveil its latest release at the Radiological Society of North America (RSNA) Annual General Meeting being held November 30 – December 4 in Chicago, IL. Circle CVI will demonstrate its newest release, cvi42v6.4. Radiology leaders know that efficiency, accuracy, and practice growth are non-negotiable. At RSNA 2025, Circle Cardiovascular Imaging invites you to experience the new cvi42 release - a solution engineered to grow your CCT and CMR business. What cvi42 can do for your practice: Reduce Reporting Times: Native integration with PowerScribeautomates transcription, minimizing error risk and freeing clinical teams to focus on interpretation rather than manual data entry. Accelerate Patient Care: In-house plaque analysis with cvi42 enables faster turnaround times, supporting timely diagnosis and allowing you to deliver a higher standard of care. Drive Confidence and Adoption: cvi42 | Vascular CT follows best practices with automated contouring, lowering barriers to using advanced CT vascular analysis - so teams adopt new capabilities faster. Increase Revenue Capture: With cvi42 | Plaque you pay for what you process at a fraction of the price of outsourcing and increase your throughput with a streamlined workflow. Elevate Value and Flexibility: Our new subscription model provides scalable access to CMR and CCT functionalities ensuring your team has unlimited access to work from anywhere. “With our latest cvi42 release, we’re helping practices unlock greater efficiency, deliver faster patient care, and build a scalable foundation for the future of cardiovascular imaging while supporting business growth” said Chris Bazinet, Chief Revenue Officer of Circle CVI. “We are excited to see how our customers respond to the latest innovations and hear from them how we are solving their challenges” Benefits for Radiology Leaders and Decision Makers: Minimized risk of errorin reporting Improved workflow efficiency, leading to reduced burnout Faster reporting speeds, translating to greater practice performance Flexibility to scale and capture new revenue streams Technology that aligns with evolving best practices and reimbursement guidelines Join Us at RSNA 2025 - Shape the Future of Cardiovascular Imaging Nov. 30 – Dec. 3 | Booth #7961, North Hall Secure your demo now - see how cvi42 can help you lead with confidence and results.
CALGARY, CANADA, OCTOBER 29, 2025 – Circle Cardiovascular Imaging Inc. (Circle CVI), a global leader in cardiovascular imaging solutions, today announced that its cvi42 | Plaque solution has received 510(k) clearance from the U.S. Food and Drug Administration (FDA) and is now available for clinical use in the United States. This innovative, AI-enabled solution allows clinicians to perform comprehensive coronary plaque analysis directly on-premise, enhancing diagnostic workflows and patient care. “The clearance of cvi42 | Plaque marks a significant advancement for cardiology departments and imaging centers,” stated Erkan Akyuz, CEO of Circle CVI. “As a secure, on-premise solution, it allows for the evaluation of coronary artery disease without the need to send patient data to an external reading service. This provides clinicians with greater control over their data, improved study processing times, and enhanced workflow efficiency.” The AI-enabled technology within cvi42 | Plaque delivers fast, accurate, and reproducible results for quantifying total, calcified, and non-calcified plaque. This detailed analysis supports more precise risk stratification and helps inform personalized treatment plans. “With the new cvi42 | Plaque, I now have immediate and interactive control over my anatomic coronary CCTA imaging analysis,” said Dr. James Thompson, DO, Adult Congenital Heart Disease at Johns Hopkins All Childrens. “Circle CVI truly comes full circle — continuing to invest, innovate, and impress by advancing imaging applications and enhancing our cardiac CTA workflow. This is foundational to CCTA’s front-line role in cardiovascular disease prevention, driving early translational impact and transformative patient care. Empowering early detection of the high-risk plaque attack.” Medicare now covers AI-enabled coronary plaque analysis from CCTA with a Category III CPT code, 0625T, and national payment set at $950under recent policy updates, alongside higher base payments for the underlying CCTA exam.With cvi42 | Plaque, cardiac imaging sites can retainmost of the reimbursement, rather than outsourcing analysis and reimbursement to external providers. AI-enabled coronary plaque analysis has been assigned a permanent Category I CPT code, 75XX6, which takes effect in January 2026. This new code, replacing previous Category III codes,facilitates national pricing and enables physician reimbursement; the AMA’s update signifies that plaque quantification is now recognized as standard clinical care in cardiovascular medicine. cvi42 | Plaque integrates seamlessly into existing CT workflows and is compatible with all major vendor systems, providing a complete solution for cardiac imaging teams. The FDA clearance reinforces Circle CVI's commitment to delivering innovative, reliable, and user-friendly solutions that empower clinicians to provide the best possible care for their patients. Discover how Circle CVI’s cvi42|Plaque can elevate your practice. Visit https://www.circlecvi.com/get-started to learn more and book a demo today.

Part 4 of 5 in Circle's Coronary Plaque series. Also read: Part 1 — How Advanced Plaque Analysis Changes the Clinical Calculus Part 2 — The IT Infrastructure Behind CCTA Plaque Analysis Part 3 — The Financial Case for Coronary Plaque Services It's Monday morning review. Throughput is off target again. Two radiologists are working through a backlog of CCTA studies from Friday. Your most experienced cardiac CT tech just submitted a PTO request for a week in July that you can't cover without asking someone else to come in. And now cardiology has sent a note asking why the plaque analysis reports are taking so long. This scenario is not unique to your department. It is the operational reality facing most cardiac imaging programs as CCTA volume grows and clinical expectations evolve faster than workflows do. Coronary plaque analysis has moved from a research capability to a clinical standard — driven by updated ACC/AHA Chest Pain Guidelines , 10-year SCOT-HEART outcomes and the ongoing SCOT-HEART 2 trial , and a growing population of patients and referring physicians who know what to ask for. Meeting that expectation with a manual workflow built for a simpler era of CCTA reporting is not a sustainable operating model. The question is not whether to offer plaque analysis. The question is how to build the workflow to deliver it without adding to a backlog that's already under pressure.

Part 3 of 5 in Circle's Coronary Plaque series. Also read: Part 1 — How Advanced Plaque Analysis Changes the Clinical Calculus Part 2 — The IT Infrastructure Behind CCTA Plaque Analysis The cardiology service line is under familiar financial pressure: rising volumes, tighter margins, growing competition from outpatient and independent imaging centers, and a capital environment that demands every major investment justify itself with a clear return. Against that backdrop, coronary plaque analysis has emerged as a meaningful financial opportunity — one with a growing reimbursement pathway, expanding referral demand, and the kind of clinical differentiation that drives patient retention. But the financial case only materializes if the program is set up to deliver the service efficiently and at scale. This is not an investment in a research capability. It is an investment in a billable, guideline-supported clinical service with a documented and growing payer footprint.

A landmark study shows that measuring how much an aneurysm sac shrinks in the first year after surgery can reliably forecast what that sac's diameter will do over the long haul — unlocking smarter, more personalised patient monitoring. The Problem with Watching Arteries Heal Abdominal aortic aneurysms — dangerous bulges in the body's main artery — kill tens of thousands of people each year when they rupture without warning. Endovascular aneurysm repair, or EVAR , is a minimally invasive surgery in which doctors thread a stent-graft through the groin to seal off the bulge from the inside, like patching a weak hose from within. It's revolutionised vascular surgery, offering patients a far quicker recovery than open surgery. But EVAR is not a cure. The sealed sac still exists inside the body, and over months and years it can change size — ideally shrinking as blood pressure is removed from it, but sometimes stubbornly staying the same or even growing. A sac that keeps expanding after surgery can signal a dangerous leak (called an endoleak ) or graft failure, either of which may require a second intervention. So, after every EVAR procedure, patients face a lifetime of periodic CT scans to check one simple thing: is the sac getting bigger or smaller? "For years, the number clinicians relied on was a single diameter measurement — essentially, how wide is the bulge? But width alone turns out to be a surprisingly blunt instrument." - Background context from the field of post-EVAR surveillance The challenge is that current guidelines require follow-up CT scans roughly every year for life, which is expensive, exposes patients to radiation, and still may miss subtle warning signs until they have become obvious on a simple diameter measurement. Researchers and clinicians have long wondered: is there a better, earlier signal we could use?

Part 2 of 5 in Circle's Coronary Plaque series. Also read: Part 1 — How Advanced Plaque Analysis Changes the Clinical Calculus When clinical cardiology adopts a new capability, IT inherits the infrastructure. And right now, coronary plaque analysis is moving from research tool to clinical standard fast enough that many IT and PACS teams are still catching up. The demand is real. The 2021 ACC/AHA Chest Pain Guidelines made CCTA a Class I recommendation for stable chest pain evaluation. More recent trial data — including 10-year outcomes from SCOT-HEART and the ongoing SCOT-HEART 2 trial — is driving cardiology programs to go further, adding quantitative plaque characterization alongside standard stenosis reporting. That means new software, new data flows, new integrations — and new complexity landing in your environment. How that complexity lands depends almost entirely on the path the department chooses. There are essentially two: a unified platform that performs plaque analysis natively, inside your existing environment — or a send-away service that moves CCTA data out of your network to a vendor cloud, runs the analysis there, and returns a result. Those two paths lead to very different IT outcomes.

Part 1 of 5 in Circle's Coronary Plaque series. Consider a familiar scenario. A 52-year-old presents with atypical chest discomfort. The stress test is borderline. The referring physician is uncertain — is this true coronary disease, or something else? Standard imaging has been done. The anatomy looks, on the surface, mostly normal. And yet something about this patient doesn't sit right. This is the case where clinicians have historically had to make consequential decisions with incomplete information. Escalate to invasive angiography and risk an unnecessary procedure. De-escalate and risk missing a vulnerable plaque that hasn't yet caused significant stenosis — but will. Coronary artery disease doesn't announce itself neatly. A substantial share of acute coronary events occur in patients with non-obstructive coronary disease — lesions that would not have triggered revascularization on a standard angiogram. The stenosis grade has always been an imperfect surrogate for risk. What matters is the plaque itself: its composition, its burden, and its vulnerability. Advanced CCTA plaque analysis changes that calculus.

The Effort, Risks, and Why It’s Worth It Quantifying the Effort of a Single Platform Learning a new (or deeper) way of working Even for existing cvi42 users, full standardization across cardiac imaging means: Adapting to new modules or modalities. Rethinking how you structure reading lists when more work is visible in one place. Helping develop shared templates and protocols. It’s completely normal to see a temporary dip in productivity when something new is introduced. Our brains are wired for loss aversion: we tend to focus more on what we might lose than on what we could gain. Recognizing that bias helps put the slowdown in perspective: it’s not a setback, it’s just part of the process that leads to long‑term progress.

Local Processing for Complete Data Security When cvi 42 processes imaging data, everything takes place within the customer’s secure environment. All image data and derived results are managed locally, whether on a hospital workstation or through a customer-managed server installation. No data is ever transmitted outside the institution. This architecture ensures compliance with strict hospital IT policies and data protection frameworks. For clinical users, this means AI-powered results without any compromise to data privacy or network security. The Circle AI Engine: Trained, Validated, and Frozen “Each of the AI models powering cvi42 is architected and developed within Circle’s controlled research and development environment. Circle’s data science and clinical AI research teams use diverse and representational datasets to train and validate each algorithm. The process typically involves supervised learning, where the AI learns to recognize patterns and structures such as the left ventricle, myocardium, or aortic root by comparing its results to expert-annotated data. Once performance meets clinical and regulatory standards, the AI model is locked, “frozen” and encrypted during its integration within cvi42. This means the model’s behavior is fixed, it does not continue to learn or change once deployed at a customer site. The model you use in cvi 42 is the validated version approved for clinical use, ensuring consistent and reproducible results across all installations. No Learning from Customer Data It is important to clarify: the AI in cvi 42 does not learn from any data processed at the customer site. The algorithm applies its pre-trained parameters to each image set locally. It does not store patient data, send information externally, or modify its internal model based on what it sees or whether a user edits its outputs. Each analysis is isolated, ensuring the AI’s decisions remain consistent and the patient’s information stays protected within the facility’s network. How the AI Analyzes Medical Images At a technical level, cvi42’s AI is a deep learning-based image analysis engine trained to recognize and segment cardiac anatomy on MR and CT images. Primarily using convolutional neural networks, it performs pixel- or voxel-level classification to delineate key structures, including the endocardial and epicardial borders. These segmentations enable the measurements of clinically relevant metrics such as chamber volumes, ejection fraction, and myocardial mass. This process mimics how expert readers would interpret the same dataset, but it happens in seconds and with objective consistency across cases. Designed for Trust, Built for Performance AI in cvi 42 is designed to automate routine analysis while keeping clinicians fully in control. Users can review, adjust, and approve AI-generated contours as needed, ensuring that results always meet their clinical standards. Combined with local data processing, frozen AI models, and Circle’s rigorous training pipeline, this approach delivers accuracy and reliability without ever compromising patient privacy.

Clinical Wins and Daily Practice Introduction A single cardiovascular imaging platform like Circle’s cvi42 changes daily work for cardiologists and radiologists from “tool juggling” to focused clinical practice. But it also asks for effort and carries real, though manageable, risks. Seeing this change from your perspective, the people interpreting images and shaping programs, makes it easier to decide whether adopting a unified platform is worthwhile.

For years, the Coronary Artery Calcium (CAC) score has been the gold standard for a quick, non-invasive look at heart disease risk. It’s a vital tool that has helped millions of patients understand if they have "hardening of the arteries." But while a calcium score tells us that plaque is present, it only tells part of the story. As medical technology evolves, we are moving beyond simply identifying the presence of calcium to a much more detailed understanding of heart disease. With the advent of AI-enabled coronary plaque analysis, such as cvi42 | Plaque , patients and physicians now have access to a deeper level of insight that was previously impossible to achieve through standard screening alone. What is AI-Enabled Coronary Plaque Analysis? While a traditional calcium score measures the amount of mineralized (hard) plaque in your coronary arteries, AI-enabled plaque analysis looks at the "soft" or non-calcified plaque as well.